Outpatient Surgery of Penile Implantation
patients
Although implantation remains the cornerstone for ED solution among many urologists,1-4 many patients hesitate to receive it because it is only non-natural therapeutic modality. Those patients with severe end-coman failure who do not respond to pharmacological treatment are good candidates for penile implants. However in our opinion it is reserved for most of those patients who sustain insufficient responsiveness of venous stripping and a nonresponder to PDE-5. In recent five year we have had lesser and lesser candidate since our promising outcomes of penile venous surgery although we have had 227 consecutive cases since 1987.5 Following the clinical experience with these successful operations, with only two patients who had to be hospitalized because of their surgical course resulting from excessive body weight, we have great confidence in our performance, procedure and technique in the clinical outpatient basis in particularly after the newfound anatomy of the tunica albuginea since 1991.6-8
Anesthesia9
Topical blockage of the proximal dorsal nerve block, peripenile injection at the penile base, with crural block, and ventral infiltration with 0.8%, 50ml lidocaine solution, prepared in an aseptic steel bowel, pre-rinsed with epinephrine,10 via a 10 ml syringe. Topical infiltration will be expanded to the tissue that is necessary and required by this prosthesis. Application of acupuncture may be necessary.
Models of Prosthesis
Use of any model should be in order, includes: semirigid penile prosthesis (mechanical or malleable one, Figure 1),5 hydraulic penile prosthesis (two-piece type: AMS Ambicor, Mentor Mark II; three-piece type: AMS 700 series [Figure 2], Mentor α 1) etc.
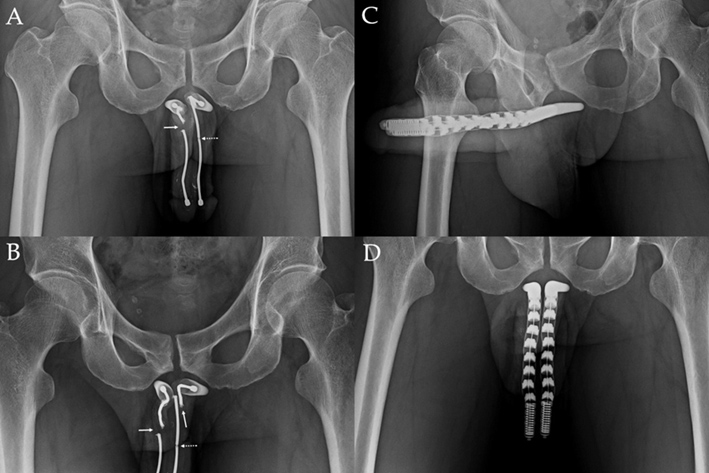
- An anterior-posterior view discloses a complete disruption (arrow) of the right wire and an incomplete disruption of the left side wire (dotted line) which is an AMS600.
- However in an oblique view, the wire of left and right corpora cavernosum is completely disrupted respectively (arrow), additionally there is an incomplete disruption (dotted arrow) in the left.
- A revision surgery was performed for implanting a malleable prosthesis "Spectra". This anterior-posterior view discloses a sound implantation.
- This oblique view further demonstrates prosthesis in situ.
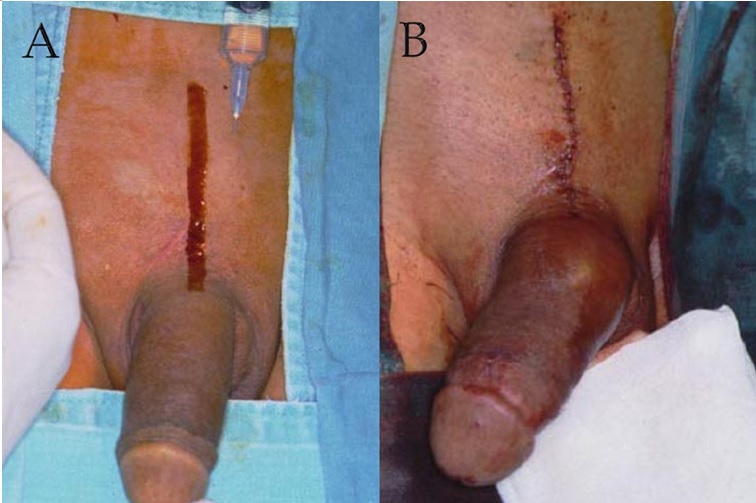
- The pubic longitudinal incision is longer than usual in order to implant the water reservoir within retropubic space. Injecting needles shall be introduced as quickly as possible to avoid intolerable pain it may occur to the patient.
- The surgery is operated under local anesthesia on outpatient basis. A booster injection might be necessary since the operation might last longer than 4 hours. The wound is finally stitched by using either 5-0 chromic or 8-o nylon suture.
Operation
Depending upon the preferable type of penile prosthesis, the circumcised, infrapubic or penoscrotal incision will be made. The implantation is performed after the corporotomy was made. The tunical wound is closed continuously with 6-zero nylon with interrupted suture per centimeter as required for enhancement. The overlying fascia layers and skin was finally closed with 5-zero chromic layer by layer. It is indifferent with a variety of approaches, such as retro-coronary, pubic and penoscrotal approach. The prosthesis shall be positioned in the best room in the corpora cavernosa (Figure 3).7
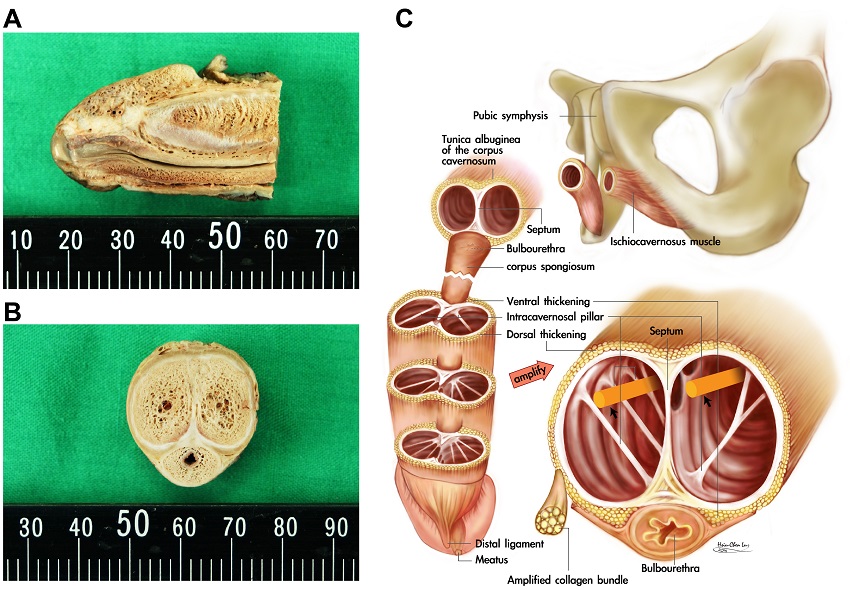
- A lateral sagittal section of the distal penis discloses the tunica albuginea of the corpora cavernosa in human penis. Both its strength and thickness varies significantly. In between a transitional membrane is clearly demonstrated outward to the intracavernosal pillars which should be laterally positioned to cylinders during penile implant. Note a stout distal ligament which was categorically overlooked before 1991.
- A cross section of the distal penis shows the thickness of the tunica albuginea varied markedly while its dorsal aspect was thicker than that of ventral one. Note the deeper-colored 300° incomplete outer longitudinal layer which is a continuation of ischiocavernosus and bulbosongiosus muscles. C. The corpora cavernosa could be divided into four spaces by intracavernosal pillars. The cylinders (purple color) of penile prosthesis were advised to house in the medial two rooms.
Anatomical position of implant
The three-dimensional structure of the human ischiocavernousus muscle as well as the bulbospongious is very dominant. Likewise its continuation tunica albuginea is a tuck envelope to house the cylinder of the implant (Figure 4). The region between the 7 to 5 o'clock positions is devoid of the outer longitudinal layer.
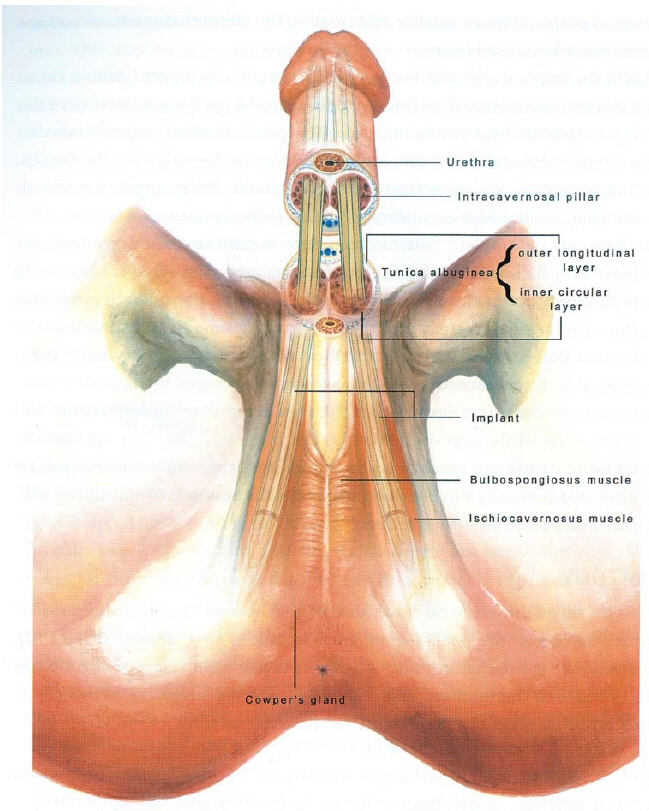
In comanic impotence, the sinusoids of the corpora cavernosa sustain severe loss of erectile capability; therefore, they ought to be replaced by an artificial implant that is housed inside and contained by the tuck tunica albuginea in which the outer longitudinal layer is a continuation part of the ischiocavernosus muscle bilaterally. The intracavernosal pillars that might be destroyed to some extent when dilatation is performed are more and more plentiful distally.
Frequently Asked Questions
- Some physicians may doubt the feasibility of a local anesthetic injection in the penis.11-14 It is in actuality quite possible, and finger-guided manipulation—in which the index finger of the assistant’s hand (usually the left hand) acts as a guide—is helpful in confirming the exact position to make the injection, particularly during the stage of the anesthetic procedure where the tissue is clearly visible. Due to the paucity of adipose tissue, the nature of layered tissue and the tuck tunica albuginea that provides a bony-like barrier are palpated. However, the key point of this operation is that the crural block requires special attention and instruction; otherwise an improper injection will inevitably follow. Therefore the cavernous other than the dorsal nerve shall be anesthetized to prevent a dilated agonizing pain to the patient.
- The crux of this procedure is to properly locate the tissue to be implanted (Figure 3). The penis is composed of three cylindrical bodies, where the sinusoids of the corpora cavernosa are surrounded and contained by the tuck tunica albuginea. Today the implant material is made of silicone that is bi-compatible and is suitable for implantation inside the sinusoids. During the dilatation, care must be taken not to damage the 5 to 7 o'clock positions of the tunica of the corpora cavernosa since this portion lies in the region where the outer longitudinal layers are scarce and weak—otherwise a dilation trauma may traumatize the weakest tunica and subsequently lead to postoperative prosthesis extrusion. This rudimentary anatomy was found in 1991 even though the modern penile prosthesis was debuted in 1950s.16
- Will the coital sensation be altered after the prosthesis is implanted? This question generally raises serious concerns among both patients and physicians. Fortunately, there will be no diminution in the coital feeling if the implant is adequately positioned as the dorsal nerve that is responsible for the feeling mounts on the tunica albuginea. In theory, then, the coital feeling will remain the same; in practice, however, some patients may perceive, and then obsess over, an apparent change in sensation.
- Will the penis remain the same size and of the same nature following implantation? Our study shows that regardless of the type of prosthesis implanted, the penile buck will expand as the implant is consistently in situ, because the extensibility of the implant is never commensurate within the sinusoid. There are several types of penile prosthesis available, such as the inflatable type, the self-contained type, the malleable form, and the mechanical one. The bulk of the former two could be reduced to some extent when the prosthesis is inactivated, but the latter two remain the same all the time. In our experience, regardless of which prosthesis the patient chooses, he becomes accustomed to it within a few months at the most.
- Is ejaculation possible with the implant? The ability to ejaculate is undiminished by the implant because ejaculatory functions take place within a near but separate anatomical space. Ejaculatory fluid is pooled in the prostatic urethra before it is expelled through the penile urethra. The implant material is housed in the corpora cavernosa and is completely segregated unless a prosthesis injury occurs.
- Is it easy to remove the implant if one needs it no more? Removal of the prosthesis is readily performed under local anesthesia on outpatient basis. In our professional practice we have not encountered any patient who intends to remove his prosthesis. Interestingly our study also shows that once patient undergoes an implant procedure, he will give considerable amount of care and attention to protect his prosthesis from being damaged.
- Will the implanted penis remain the same length? Some patients may complain that an implant penis is a little shorter than that of the preoperative one. This may be true, although no documentation is available so far. About 30% of our patients prompted this concern, and that some of these were solved by a newly developed elongation technique. Likewise some patients will also sustain a rather pale and colder glans after implantation. A penile enhancement surgery can elongate the copulatory portion of the penis via two Z-plasties on the pubic region and penoscrotal junction respectively. Again this operation is done under local anesthesia and outpatient basis.15
- Local anesthetic is recommended to irrigate within the corpora cavernosa.1,2,4,13,14 However we advise not only to avoid this procedure, but also be cautious not to puncture into sinusoid through the tunica, particularly if an implant is in situ and a booster injection is necessary when patient has regained some pain intraoperatively. Hence this avoids possible complications of dizziness, palpitation as well as nausea and vomiting.
- Routinely 5 to 6 acupuncture needles are applied to cover 3 standardized acupoints: Hegu (LI 4), Neiguan (PE 6) and Quchi (LI 11) bilaterally.11 The acupoint of Hegu is located at the highest point of the prominence if the thumb and the index finger are kept adducted. The Neiguan point is positioned 3-finger-bredth proximal to the midpoint of the volar transverse carpal crease, between the flexor carpi radialis muscle and the palmaris longus tendon if the forearm keeps supine. The Quchi point is at the lateral end of the transverse cubital crease with the elbow flexed at a right angle. After the acupuncture most patients shift their attention more to these acupoints rather than their operation. Pethidine injection is no longer necessary.
- Local anesthesia on an outpatient basis for penile implant is very promising, and this method of penile crural block proved to be a reliable, simple and safe method with less complication. It offers the advantages of less morbidity, with concern of patient's privacy while allowing them return to their normal activities rapidly.9
- Will the implant trigger an alarm when one passes through a security check-point? As the implant material gets better and better with the metal portion getting smaller and smaller, the alarm that it evokes will not be a problem in the future. Although we have only provided penile implantations to 251 patients since 1988, studies of both rudimentary penile anatomy and erection physiology are inspired by numerous patient questions and incidents.17-21 Would prosthesis survival rate be only some 60% in 15 years? Our data fails to agree it; among 195 males with malleable or mechanical prosthesis, we have documented only one case of prosthesis loss.
References
- Kaufman JJ. penile prosthesis surgery under local anesthesia. J Urol, 128: 1190, 1982
- Scott FB. Outpatient implantation of Penile Prostheses under local anesthesia. Urol Clin North Am, 14: 177, 1987
- Brown TC, Weidner NJ and Bouwmeester J. Dorsal nerve of penis block--anatomical and radiological studies. Anaesth Intensive care, 17: 34, 1989
- Dos Reis JM, Glina S, Da Silva MF et al. Penile prosthesis surgery with the patient under local regional anesthesia. J Urol, 150: 1179, 1993
- Hsu GL, Chen HS, Huang SJ. Does tunica anatomy matter in penile implant? Transl Androl Urol 2014; 4(4):406-412. doi: .3978/j.issn.2223-4683.2014.03.04 (Correspondent and Principal author)
- Hsu GL, Brock G, Martinez-Pineiro L, von Heyden B, Lue TF, Tanagho EA. Anatomy and strength of the tunica albuginea: its relevance to penile prosthesis extrusion. J Urol, 151: 1205-8, 1994.
- Hsu GL, Hsieh CH and Chen SC. Human penile tunica albuginea: Anatomy discovery, functional evidence and role in reconstructive and implant surgery. Glo. Adv. Res. J. Med. Med. Sci. 2014; 3: 400-407. (Correspondent and Principal author)
- Hsu GL, Hsieh CH, Wen HS, Hsu WL and Chen CW. Anatomy of the human penis: The relationship of the architecture between skeletal and smooth muscles. J Androl. 25: 426-431, 2004. (Correspondent and Principal author)
- Hsu GL, Hsieh CH, Wen HS, Chen SC, Chen YC, Liu LJ, Mok MS and Wu CH. Outpatient penile implantation with the patient under a novel method of crural block. Int J Androl. 27: 147-151, 2004. (Correspondent and Principal author)
- Bernards CM and Kopacz DJ. Effect of epinephrine on lidocaine clearance in vivo: a microdialysis study in humans. Anesthesiology, 91: 962, 1999
- Hsu GL. Peyronie's disease. In: APSIR BOOK on Erectile Dysfunction, 1st ed. Edited by Kim, Y. C. and Tan, H. M. Malaysia: Pacific Cosmos Sdn Bhd, chapt. 18, pp. 200-212, 1999
- Hsu GL, Zaid UX, Hsieh CH, Huang SJ. Acupuncture assisted regional anesthesia for penile surgeries. Transl Androl Urol. 2013; 2: 291-300. doi: 10.3978/ j.issn.2223-4683.2013.12.02 (Invited, correspondent and Principal author)
- Serour F, Mandelberg A and Mori J. Slow injection of local anesthetic will decrease pain during dorsal penile block. Acta Anaesthesiol Scand, 42: 926, 1998
- Ghanem H and Fouad G.:Penile prosthesis surgery under local penile block anesthesia via the infrapubic space. Int J androl, 23: 357, 2000
- Hsu GL, Hill JW, Hsieh CH, Liu SP and Hsu CY: Venous ligation: A novel strategy for glans enhancement in penile prosthesis implantation. BioMed Res Int Volume 2014, Article ID 923171, 7 Pages, 2014.http://dx.doi.com/10.1155/2014/923171 (Principal author & corresponding author)
- Hinman F Jr. Penis and male Urethra. In Atlas of uroSurgical Anatomy. Chapt 16. Philadelphia: W.B. Saunders, 1993; pp. 432-433.
- Hsu, G-L. (2018). Erection Abnormality. In M. K. Skinner (Ed.), Encyclopedia of Reproduction. vol. 1, pp. 382–390. Academic Press: Elsevier. http://dx.doi.com/10.1016/B978-0-12-801238-3.64374-X
- Hsu, G-L., & Liu, S-P. (2018). Penis Structure. In M. K. Skinner (Ed.), Encyclopedia of Reproduction. vol. 1, pp. 357–366. Academic Press: Elsevier. http://dx.doi.com/10.1016/B978-0-12-801238-3.64602-0
- Hsu, G-L., & Lu, H-C. (2018). Penis Structure—Erection. In M. K. Skinner (Ed.), Encyclopedia of Reproduction. vol. 1, pp. 367–375. Academic Press: Elsevier. http://dx.doi.com/10.1016/B978-0-12-801238-3.64603-2
- Liang, J-y., Chang, H-C., & Hsu, G-L. (2018). Penis Endocrinology. In M. K. Skinner (Ed.), Encyclopedia of Reproduction. vol. 1, pp. 376–381. Academic Press: Elsevier. http://dx.doi.com/10.1016/B978-0-12-801238-3.64604-4
- Huang, P-C., & Hsu, G-L. (2018). Vascular Surgery for Erectile Dysfunction. In M. K. Skinner (Ed.), Encyclopedia of Reproduction. vol. 4, pp. 427–436. Academic Press: Elsevier. http://dx.doi.com/10.1016/B978-0-12-801238-3.64804-3
 Images on this webpage are licensed under a CC Attribution-ShareAlike 4.0 International License.
Images on this webpage are licensed under a CC Attribution-ShareAlike 4.0 International License.